Coverage is not enough: why universal health coverage must tackle inequality
Universal health coverage – a central target of the SDGs – seeks to guarantee access to essential health services without financial hardship. Achieving it, however, requires confronting the inequalities in access and quality that coverage alone cannot resolve
Health — Global

Author
Tobias Schillings
Postdoctoral Researcher, Technical University of Munich; Research Associate, University of Oxford
Universal health coverage (UHC) has become one of the central ambitions of the global development agenda. Over recent decades, governments have expanded insurance schemes, broadened benefit packages, and increased investment in primary care. Measured against the headline indicators of Sustainable Development Goal (SDG) Target 3.8, the commitment to UHC has produced real progress.
But expanding who is formally covered is not the same as building truly universal health systems.
In many countries, formal enrollment tells us little about what people actually receive when they seek care. A person may be formally entitled to services while still facing under-resourced facilities, long waiting times, unavailable medicines, or out-of-pocket payments that risk pushing them into poverty. Meanwhile, those with the financial means can often bypass inadequate public provision by turning to private alternatives that are better resourced and of higher quality.
These inequalities are not limited to a simple public–private divide. Even within public systems, access and quality may vary sharply by region, occupation, income, or social group. Separate schemes may offer different levels of entitlement to different populations. The result is a layered reality: more people are included in health systems, but not necessarily on equal terms.
This matters because universal healthcare is not only about whether people enter the system, but also about what kind of system they enter.
Why inequality in healthcare matters
The consequences of unequal and insufficient health systems are not abstract. Research on low and middle-income countries has shown that more than 8 million people die each year from conditions that should be treatable, and that 60 percent of these deaths are linked not to the complete absence of care, but to poor-quality care. The problem is therefore not simply that people cannot reach the health system. Often, the problem is that the system cannot adequately serve them – and that this inadequacy is unequally distributed.
But the stakes extend beyond health outcomes alone. Where healthcare systems are stratified by ability to pay, they entrench poverty traps and deepen economic inequality. They also erode the institutional trust on which inclusive societies depend. When people experience public services as unreliable or unequal, their confidence in the state – and in shared social institutions more broadly – diminishes. This is why UHC must be understood as part of the wider SDG agenda: unequal health systems do not merely fall short on health. They undermine the foundations of equitable and resilient societies.
Universalism is more than coverage
Addressing this reality requires a more precise understanding of what it means for a health system to be universal. The question is not only whether people are enrolled, but what they receive when they seek care – and whether what they receive depends on who they are.
A useful way to frame this is to ask three questions simultaneously:
- Who is covered?
- What level and quality of services do they actually receive?
- Is access distributed equitably across social groups?
This distinction matters because health systems can expand in very different ways. One country may increase formal enrollment while offering only limited and underfunded services to large parts of the population. Another may achieve broad access but continue to tolerate major differences in quality between regions, occupations, or income groups. A third may combine wide coverage with adequate public support and relatively equal access to care.
All three may appear to be moving toward UHC, but they are not equally universal. Understood this way, universalism is a matter of degree rather than a binary achievement. A genuinely universal health system progressively narrows the gaps in access, quality, and financial protection – rather than simply widening the tent of formal enrolment.
What the Healthcare Universalism Index shows
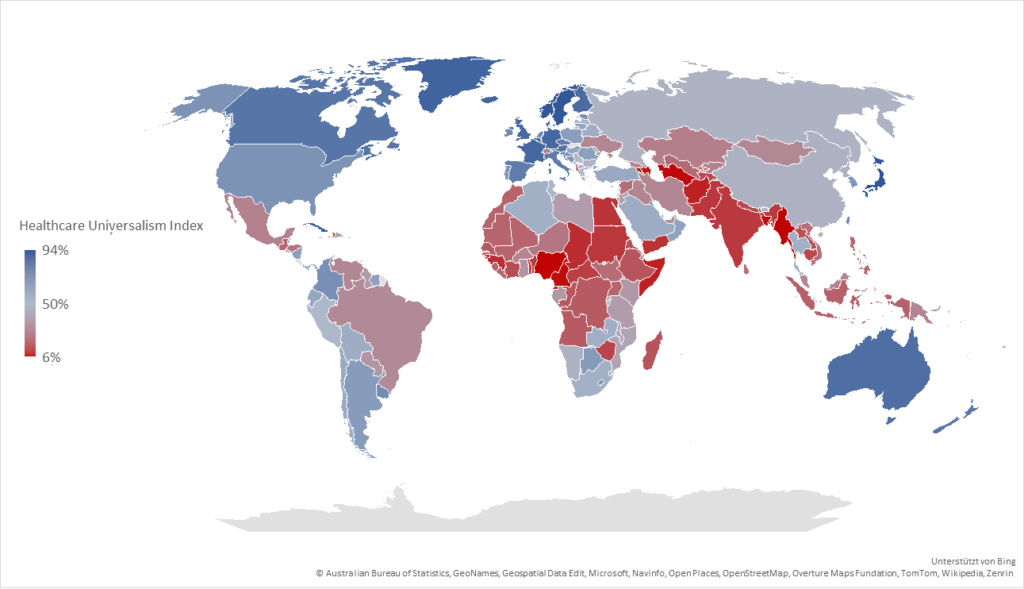
To measure these dimensions, Diego Sánchez-Ancochea and I developed the Healthcare Universalism Index (HUI), launched as part of the UN Development Programme’s Special Report on Human Security. Rather than tracking enrollment alone, the HUI combines three dimensions – coverage, generosity, and equity – to ask whether health services are adequately funded and equitably distributed across the population.
Our research (The Role of Healthcare Universalism in Advancing Human Security) shows that the global picture is more nuanced than a simple story of success or failure. Since the mid-1990s, healthcare universalism has improved substantially across many parts of the world. Progress in coverage and access has been real and meaningful – and it challenges the assumption that poorer countries must wait for economic growth before expanding health services. But the same evidence exposes persistent gaps in the dimensions that matter most for equality. Coverage has expanded; generosity and equity have lagged. In lower-income countries, limited public investment remains the central structural barrier, with basic entitlements often existing on paper without the resources to make them real. In richer countries, high average coverage can conceal persistent inequalities driven by marketization and fragmented provision. Overall, the world has moved toward broader inclusion, but not consistently toward greater equality in healthcare.
Figure 1: Healthcare Universalism Index 2023
From evidence to policy: the challenge of segmentation
The central policy implication is not simply to do more of what has worked so far. Expanding access without addressing how systems are structured risks consolidating a pattern in which coverage grows while inequality persists.
The most underappreciated obstacle here is segmentation. Many health systems have expanded by layering separate schemes on top of one another – different entitlements for different groups, separate benefit packages for formal and informal workers, parallel tracks for the insured and the uninsured. These arrangements can raise headline coverage figures while quietly deepening the inequalities that matter most. The structure of the health system can end up reproducing the structure of society.
Moving toward more equal systems therefore requires more than investment – it requires building common frameworks: shared benefit packages, integrated service provision, and a sustained commitment to quality alongside coverage. Reducing out-of-pocket spending remains a direct test of whether access still depends on ability to pay. And tracking enrollment alone overstates success; monitoring frameworks that capture equity and quality alongside coverage are essential to holding systems accountable.
A more ambitious vision of UHC
The ambition of UHC is not simply to include everyone in a health system. It is to ensure that everyone is treated as an equal member of it. That is a harder goal. It requires sustained investment, institutional reform, and the political will to challenge arrangements that benefit those already advantaged.
But the experience of many countries shows that progress on this deeper definition of universalism is possible at all levels of development – that it is as much a matter of political choice and institutional commitment as it is of economic capacity.
If the next phase of the global health agenda is to succeed, it will need to hold both ambitions at once: expanding who is covered, and transforming what coverage means. The SDGs call for a world in which no one is left behind – not only in principle, but in practice. On health, that means moving from a politics of enrollment to a politics of equality.

Related articles

When work separates mothers and babies, everyone pays the price
Mothers are encouraged to breastfeed, yet too often expected to do so within work systems built around separation. If we want to improve breastfeeding rates, those systems must change – through stronger legislation on workplace responsibilities, flexible working, and care arrangements that allow mothers and babies to stay together


Redefining sustainable water management for a water-scarce world
Through innovation, foresight, and rigorous alignment with global standards, Dubai Electricity and Water Authority (DEWA) is pioneering a future-ready water management model that safeguards reliability, sustainability, and resilience, contributing meaningfully to the achievement of SDG 6